After we had tested the train-the-trainer courses of the DID-ACT curriculum, it was time to evaluate the quality of learning units for students. We have conducted a series of pilot studies that validated five different learning units in eight evaluation events across all partner institutions including also associate partners. We have recorded student activities in the virtual patient collection connected with the DID-ACT curriculum available for deliberate practice. In addition, we evaluated the usability of the project’s learning management system in several test scenarios.
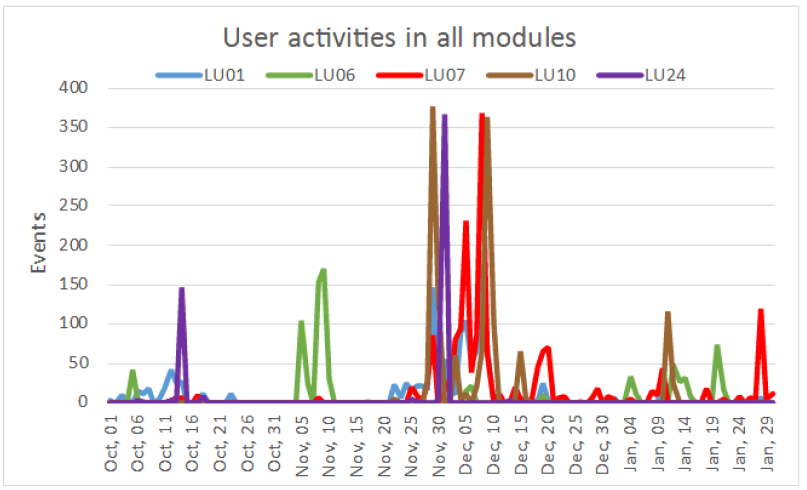
Overview about student activities in piloted learning units
Overall, students agreed to a large extent that the piloted DID-ACT learning units improved their clinical reasoning skills (average 5.75 in 7-point Likert scale). As a special strength of the curriculum students frequently named the benefit of virtual patients integrated with the learning units. Another highlight were small-group group discussions, often conducted in multinational teams which broadened their views on clinical reasoning. However, a challenge in the tested version of the curriculum implementation was navigation in the learning management system (Moodle). As a consequence, we have further analyzed these data and, furthermore, conducted a series of usability tests. These analyses and tests led to a process to address the issues wherever it is possible. We have also received several requests for modifications of the developed learning material that we will address in the next deliverable, in which we refine courses based on pilot implementation.
To ensure the quality of our curriculum’s development, our pilots accompanied a questionnaire for participants and facilitators. We are using this feedback to create necessary emphasis and/ or create a clearer final product for our learners. These responses were coupled with monitoring our chosen learning management system (LMS), Moodle, and virtual patient system, CASUS. DID-ACT’s six institutional partners took part in the evaluation by facilitating 9 pilot courses across Europe. In brief, approximately 100 teachers participated in the 5 clinical reasoning teaching topics in the train-the-trainer course pilots. Approximately half of the participants returned their evaluation questionnaires alongside 12 responses from facilitators. The results, discussed further here, coding was double-checked and disagreements were solved by consensus.
Survey tools for clinical reasoning curriculum assessment
In our pilots we made the decision to use survey-based tools for measuring the train-the-trainer (TTT) and students courses. Our goal was to capture responses using fewer questions in a way that allowed for comparison between piloted units. In the end, we used Evaluation of Technology-Enhanced Learning Materials (ETELM). This tool, developed by David Cook and Rachel Ellaway, gave us our launch pad to have questionnaires be our standard evaluation tool. This was attractive for many reasons, including facilitating implementation into our learning unit template within our LMS.
Lessons learned around evaluations for our pilot implementation
Through iteration and collaboration with a psychologist, experienced educators, and researchers, we found the following pertinent for our project and beyond:
Ensure you are using consistent language; i.e use either ‘course’ or ‘learning unit’, as pertinent to your project
Be mindful of using the word ‘practice’ as it can be interpreted many ways; i.e in DID-ACT’s case, we changed, “This learning unit will change my practice” to “This learning unit will improve my clinical reasoning”
Providing participants an option to write free-text in their native language, as a project allows
Avoid too many questions that may lead to overloading participants
Asking about years in a profession versus age provides more succinct answers for what we needed.
TTT Pilot Implementation Survey Results
We set up our questionnaires using a scale of 1 (definitely agree) to 7 (definitely disagree). The average score of responses was 5.8 when prompted with the question about whether the courses would improve the teaching of clinical reasoning. The pilots excelled in the areas of selection of topics, small group discussions, the facilitators, and inter-professional learning opportunities. Growth was suggested in the areas of technical navigation of the LMS, assessment and feedback on process, and content that was tailored more to professions other than physicians.
Analysis of Pilot Implementations
The survey questionnaires were analyzed on Microsoft Excel where, using quantitative methodology, we calculated the descriptive statistics. In contrast, for open-ended responses, we performed a content analysis. Participant utterances were coded with the categories proposed in D3.2 (Didactical, Content, Technical, Interaction/ Collaboration, Implementation/ Time, Implementation /Facilitators). As well, we extended by adding three more categories (Content/Assessment, Overall and Others). All data was processed anonymously with each statement being set as positive, negative, or neutral.
Overall, the TTT pilot implementations were a success as well as were our efforts in evaluating them. We will implement constructive feedback applicable to other learning units as we continue to develop them. Alongside this, we will return to the original pilot implementations and amend what needs to be improved. You can read a more detailed overview of D5.2 Evaluation and analysis of learner activities during these TTT pilot implementations here.
Looking back at our last chunk of time in the DID-ACT project, we have a lot to be proud of and a lot to look forward to. One of the most exciting and hands-on aspects of this clinical reasoning curriculum launch is where we are right now: Pilot Implementations.
Train the trainer course on clinical reasoning
In our latest report published, Pilot implementations of the train-the-trainer course, we focused on the train the trainer learning units for our curriculum. These pilots were valuable and insightful in terms of helping the team iron out kinks in content, strategy, communications, etc. Overall, we had 7 courses that covered 4 different clinical reasoning topics up until the end of October. We are pleased to share that this made for a total of 69 participants who included professions such as medicine, nursing, paramedics, basic sciences and physiotherapy, from various partner-, associate-partner, and external institutions. We also had student participants. Overall the feedback was very positive. Next up is to take this feedback given and implement it into the curriculum.
Quality criteria for pilot implementations
Our quality criteria, which we were successful in achieving, were the following:
More than 50 participants from partner and associate partner institutions, as well as external participants
Covering a wide range of topics of the train-the-trainer courses that fit to the partner faculty development programs
Piloting of at least two same learning units by 2-3 partners
Thoroughly evaluated based on questionnaires for participants and instructors and learning analytics (in alignment with WP5).
Methods for a train the trainer implementation
We used our chosen learning platform Moodle to host our blended learning curriculum. There were several steps taken to ensure implementations were as smooth and consistent as possible. It began with a succinct planning phase.
Planning phase
Most of the train-the-trainer courses were chosen in tandem with their student curriculum counterparts. This was done intentionally so that trainers would be adequately prepared themselves to teach the students. Each institution chose their learning unit based on their individual needs and requirements. During this time, the consortium met on a regular basis to plan and ensure that quality criteria would be met. As well, alongside doing pilots within our consortium, we elected to have external participants as well for external applicability.
Implementation phase
The implementation happened differently at each institution and recruitment ranged from emails to specific cohorts to full public university call. During this time, each member was supported by Instruct to ensure that course access, structure of the pilots, and required facilitator resources were accessible and clear. This included a roadmap on how to use the Moodle platform as that was highlighted previously as an area with need support. Differences were also du to use of course forums and analysis of feedback within the learning platform.
Analysis and feedback phase
One of the deliverables for work package 5 was an evaluation questionnaire, as well as an analysis of the usage data. The former was given to participants at the end of the learning unit. Alongside this evaluation, each facilitator was given a short template to fill in for more qualitative reporting on their experience. Each of the responses was categorized and discussed together.
Results
In the end, we piloted 4 interprofessional sessions and 3 with external participants. Feedback was generally positive and otherwise anything that could be termed as less than ideal is being used as constructive feedback for further refinement. Our biggest wins were that the interactive aspect was found to be highly valuable and the facilitators from varied professions was appreciated. Our constructive feedback was around Moodle and Casus being unclear as tools, too little time, teaching topic vs teaching how to teach was a crunch, as well as how the conversation veered toward medicine due to the unbalanced participant professions (i.e too many phyisicans versus physiotherapists in one group).
Pilot implementation conclusions
Overall, the consortium deems this round of clinical reasoning pilot implementations a success. There are points we need to work on, such as Moodle clarification, additional tutorial video was already produced, and time constraints, which will all be addressed in the coming review period for the learning units. What’s more, the consortium will be delving during to the conclusions on the didactical and content-level for the learning units via the evaluation results reported in D5.2. These will all be brought forward during the overall revisions and improvements slated for D3.3 which begins in January 2022.
Virtual Patients (VPs)
The virtual patients integrated into the DID-ACT learning units are partly taken from the EU-funded project iCoViP and form the collection for deliberate practice. The virtual patients are freely accessible via the CASUS system at https://crt.casus.net and a description of available VPs with key symptoms and final diagnoses is available in this blueprint. Thus, you can choose VPs suitable for your students and also offer them the whole collection for longitudinal and deliberate practice.
Participants: Medical educators
Learning units: Person-centered approach and the role of patients Level: Teacher
Description: Offered as part of the faculty development to faculty educators. Mode: Part to the faculty development program with emphasize on the educational potential of clinical reasoning teaching techniques
Technical Integration: Access to the DID-ACT Moodle, synchronous sessions were held via the virtual platform NewRow.
Learning units: What is Clinical Reasoning and Models Level: Teacher
Description: Offered as additional faculty development opportunity to staff members of the Medical Education Department. Mode: Option / additional part to the faculty development program with emphasize on the educational potential of clinical reasoning teaching techniques
Technical Integration: Access to the DID-ACT Moodle via EduGain, synchronous sessions were held face-to-face.
Tips & Tricks: Give participants time to familiarize themselves with the learning material between the sessions. Do not put too much in one day - better to meet twice for shorter sessions. Face-to-face sessions lead to more productive discussions than Zoom meetings. Focus on discussion with the audience and on examples from practical teaching to illustrate the learning objectives.
Participants: Multi-professional educators
Learning units: Differences and similarities in clinical reasoning among health professions Level: Teacher
Description: Offered as part of the faculty development program, it was held as a blended learning course with the synchronous phase online. Mode: Part of the faculty development program with certificate
Technical Integration: Access to the DID-ACT Moodle via EduGain, synchronous sessions were held online via Zoom.
Tips & Tricks: Give good practical information how Moodle works and how the participants can find and work with the different assigments of the learning unit. Emphasize the importance to the participants to work with the different individual tasks, as the discussions will be more interesting and fruitful. Also important that all the participants from different occupations feel comfortable to meet and that they all are a part of the discussion. This is an important and maybe the primary task for the facilitator!
Participants: Multi-professional and international educators
Learning units: Clinical Reasoning teaching and assessment & What is Clinical Reasoning and Models Level: Teacher
Description: Offered as optional learning unit for participants of the Master of Medical Education (MME) program in Bern/Switzerland. Mode: Part of the faculty development program with certificate
Technical Integration: Access to the DID-ACT Moodle via EduGain, synchronous sessions were held face-to-face.
Tips & Tricks: To foster a valuable learning experience it is indispensible to provide good case examples that are tailored to the needs and experiences of the participants, so that they can relate to their prior knowledge. Thus, the provided examples in this learning units might need some adaptations for your target group of educators.
Participants: Multi-professional educators across German-speaking coutries
Learning units: Differences and similarities in clinical reasoning among health professions Level: Teacher
Description: Offered as part of the faculty development program at the University of Augsburg, but open to participants from Germany, Austria, and Switzerland. It was held as a blended learning course with the synchronous phase online. Participants were eager to exchange their experience and disucss their views across institutions and professions. Mode: Part of the faculty development program with certificate
Technical Integration: Access to the DID-ACT Moodle via EduGain, synchronous sessions were held online via Zoom.
Tips & Tricks: To foster a valuable interprofessional experience the participants should represent a balanced mix of professions and also ideally the facilitators should at least represent two different professions. This allows a good discussion and also guarantees that the small groups can work interprofessionally. Our experience with a less-balanced group composition was that the over-represented profession dominates the discussions and it was quite difficult to counter-balance this.
Target group: Medical students in year 2
Learning units: Person-centered approach to clinical reasoning Level: Novice
Description:The Learning Unit was run as an extra-curricular session as a virtual class. The facilitators were trained on this topic by attending the Train-the-trainer learning unit on "Person-centered approach and the role of patients". Mode: Extracurricular activity
Technical Integration: Access to the DID-ACT Moodle via EduGain, synchronous sessions were held online via NewRow.
Tips & Tricks: Learning objective cross-referencing with the existing curriculum helps identify the level of integration. Encouraging and helping students to get familiar with Moodle before the session facilitates a smooth integration of the asynchronous phases.
Target group: Medical students in year 4 and 5
Learning units: Generating differential diagnoses and deciding about final diagnoses Level: Novice
Description: The learning unit was integrated into a pediatric emergency department clerkship with a relation to virtual patients already used in this clerkship. Facilitators were trained by attending the train-the-trainer unit on "Information gathering, Generating differential diagnoses, Decision making, and Treatment planning". Mode: Part of a regular curricular activity
Technical Integration: Access to the DID-ACT Moodle via EduGain, synchronous sessions were held face-to-face.
Tips & Tricks: Integration into clerkships works well, especially with a relation to already used content.
Target group: Medical students in year 1-6
Learning units: All 25 learning units of the DID-ACT curriculum Level: Novice - Advanced
Description: Longitudinal integration of the DID-ACT learning units into a clinical skills & communication course with the following suggested distribution across years: Year 1: What is Clinical Reasoning, Person-centered approach to clinical reasoning, Health profession roles in clinical reasoning, and Biomedical Knowledge & Clinical Reasoning. (Required time in curriculum ca. 5 hours / semester) Year 2: Dual Process Theory, Illness scripts, Collect and prioritize key clinical findings/problems, and What is clinical reasoning and How can theories be put into practice (Intermediate). (Required time in curriculum: ca. 4 1/2 hours/semester) Year 3: Generating differential diagnoses and deciding about final diagnosis, Biases and cognitive errors - an Introduction, Analyzing and avoiding errors. (Required time in curriculum: ca. 4 1/2 hours/semester) Year 4: Using the Outcome Present State Test Model, Developing a treatment plan, Metacognition, reflection and models for reflection, Collaboration of health professions in Clinical Reasoning (Intermediate). (Required time in curriculum: ca. 6 hours/semester) Year 5: All remaining intermediate learning units: Shared Decision Making in Clinical Reasoning, Decision Support Systems, Ethical aspects - patient management and treatment, Uncertainty. (Required time in curriculum: ca. 5 hours/semester) Year 6: All 6 advanced learning units: Collaborate with others in clinical reasoning, Decision Support Systems, Biases and cognitive errors, Uncertainty, Metacognition, reflection and models for reflection, Analyzing and avoiding errors. (Required time: ca. 6 hours / semester. Final year students often have a day/week off from clinical work so these days could be used for DID-ACT learning units and optional participation in the train-the-trainer units) Years 1-5: Virtual Patients (VPs) as additional deliberate practice activities in increasing number and complexity (e.g. starting with 5 VPs (=ca. 1.5 hours)/semester) in Year 1 and increasing to 10 VPs/semester) in Year 3-5. Mode: Integrated into a clinical longitudinal course that runs from year 1 to 6 resulting in a total of 2.4 ECTS.
Technical Integration: Access to the DID-ACT Moodle via EduGain, synchronous sessions face-to-face or online.
Tips & Tricks: Alining a longitudinal curriculum with curricula of other health professions remains a challenge and requires careful and early planning, but the asynchronous phases might be a good starting point for interprofessional teaching sessions. The VPs can be quite easily aligned with other curricular courses e.g., based on key symptoms.
Target group: Medical students in year 3
Learning units: Person-centered approach to clinical reasoning Level: Novice
Description: The learning unit was integrated into the Laboratory Training of Clinical Skills. This course consists of six face-to-face meetings for groups of around 10 students. Within the meetings the students discuss various topics related to communication skills and person-centered approach. The fifth of the six meetings of the course was replaced by the DID-ACT learning unit. Students could then refer back to this learning unit during final session of the course. Mode: Part of a regular curricular activity
Technical Integration: Access to the DID-ACT Moodle via EduGain, synchronous sessions were held face-to-face. If possible, a uniform technology to provide access to the online resources in the class (using university tablets in our case) and support of the technical staff on-site was helpful to lower the technical barrier.
Tips & Tricks: Changing of the standard format of classes is interesting and motivating for the students. Virtual patients are a tool to present authentic clinical scenarios which are appreciated by the students. A blend of role-play and virtual patients allows students to take advantages of the two methods to reach the learning objectives.
Target group: Medical students in year 2 and nursing students in year 3 across Europe
Learning units: Collaboration of Health Professions in Clinical Reasoning Level: Intermediate
Description: This learning unit was implemented with , aside from clinical reasoning, tow additional objectives: 1) providing internationalization experience for students without traveling. 2) Deepening the knowledge of one's own professional roles and responsibilities and knowledge of another profession . Mode: Extra-curricular interprofessional learning session with international participants
Technical Integration: Self-registration on DID-ACT Moodle, synchronous sessions via zoom.
Tips & Tricks: Facilitators running this course and supporting the discussions should be careful about supporting and encouraging all the participating professions' perspectives.
Target group: Medical students in year 1 and 2 (preclinical) across Europe
Learning units: Introduction into Clinical Reasoning & Health profession roles in clinical reasoning Level: Novice
Description: The course was offered as a blended learning module to students from different medical schools in Europe as an international elective. Synchronous phases were held online via Zoom. The international aspect was very motivating for students and they learnt a lot from each other by exchanging their perspectives and how they are taught clinical reasoning vaspects. This teaching mode could also be implemented as an activity to welcome or prepare new Erasmus students. Facilitairs were trained by attending the train-the-trainer learning unit on "Differences and similarities in clinical reasoning among health professions". Mode: Elective course
Technical Integration: Self-registration on DID-ACT Moodle, synchronous sessions via zoom and use of Padlet for interactivities.
Tips & Tricks: The organization with the registration of students was a bit complex, so, we suggest just setting dates and let students book. Allow enough (more time) for discussion and introduction rounds as participants do not know each other and are eager to hear and learn from peers at other schools and countries. Ideally, this session could also be held interprofessionally, however, it makes the finding of suitable dates even more complex.
How to teach synchronously in a virtual setting
You need a reliable camera, microphone, and virtual platform and be familiar with its features, such as whiteboard, chat, polling, breakout rooms, etc.
At the beginning establish communication rules, e.g. whether participants should raise their (virtual) hand, use the chat, and/or just speak. Also, we recommend asking participants to turn on their camera
For small group work break out rooms work very well, just be clear about the tasks the groups should work on prior to dividing them into the groups.
For collaboration the use of integrated virtual whiteboards or other platforms such as Padlet are very useful. Just make sure prior to the session that you have everything setup and the links at hand, e.g. to post them in the chat.
Allow a bit more time for starting the session and the group works as there might be participants who are not familiar with the platform or technical problems might occur.
How to motivate unprepared participants
Make clear that the asynchronous assignments are a core part of the course and that its content will not be repeated. Even if it is difficult, stick to that when starting the synchronous teaching session.
If you expect unprepared participants, you can start the session with a student-centered group exercise mixing prepared and unprepared students to increase peer-pressure and make them realize that being unprepared does not feel good.
Use the introductory or closing quizzes / tests so that participants can self- assess whether they have the required knowledge and you as a facilitator can see the level of knowledge and preparation of your participants.
Further recommended reading:
Hege I, Tolks D, Adler M, Härtl A. Blended learning: ten tips on how to implement it into a curriculum in healthcare education. GMS J Med Educ. 2020;37(5):Doc45. (Article)
How to involve participants with different levels of experience
To account for such different levels, we recommend making use of the asynchronous preparatory phases which also include introductory quizzes in which participants can self-assess their prior knowledge and you as a facilitator can assess the differences within your group. Participants with less prior experience can also be guided to additional preparatory resources.
Encourage participants to work in pairs or small groups when preparing so that they can help and learn from each other. You could even facilitate this by dividing them into groups with different levels of experience.
Similarly, during the synchronous phases, we recommend forming groups with participants different levels of experience and emphasize the peer support aspects of such group activities.
We also recommend starting with rather smaller groups and allow more time than stated in the course outlines, if you expect a heterogenous level of experience. This way you can better manage this challenge.
Encourage your participants to ask questions, emphasizing that nobody knows everything and that it is important for learning to ask questions.
Especially in the train-the-trainer course you might have to deal with over-confident participants, who especially in an interprofessional setting can dominate the group. This is a complex cultural challenge, but you could try to establish (and follow) communication rules at the beginning of a session.
How to address potential overlaps or redundancies
Identify what is already included and what is missing in your curriculum related to clinical reasoning outcomes and compare it to the DID-ACT blueprint. Prioritize learning outcomes that are not yet covered but regarded as important.
Identify activities, resources, or teaching sessions with similar learning outcomes that might be in need for change anyway because of low evaluation results, teachers or students struggle with it. These could be suitable for adding or replacing parts with DID-ACT activities.
Ask teachers and students about overlaps and gaps they see in their teaching / learning of clinical reasoning and where they struggle. This could also be done by a reflection round after related teaching activities in the curriculum
Although ideally a longitudinal integration is aimed at, we recommend to starting small with a pilot implementation to gain experience and develop a show case.
How to teach in an interprofessional setting
Allow for enough time prior to the teaching for the organization and motivation / encouragement of stakeholders and participants
Allow for enough time and guidance during the course so that the participants from the different professions can get to know each other and their professions and discuss their different perspectives. This might mean that you need to calculate some extra time in addition to the suggested duration of the learning unit.
There may be a different understanding of clinical reasoning in the different health professions, so we recommend making participants aware of this. You could for example use and adapt activities from the learning units on the health profession roles to facilitate this.
Courses in an interprofessional setting should not come too early in the curriculum (not before professions have formed their own professional identity - however, this also depends on the aim of the course).
Make sure you have enough participants from different professions. If possible, the facilitator could divide the participants in smaller groups with an equal distribution of professions.
Similarly, you need an equal distribution of facilitators / facilitators from different professions.
Develop customized learning materials considering the different professions. If needed you can adapt the material and activities provided in the DID-ACT curriculum.
Further recommended reading:
van Diggele, C., Roberts, C., Burgess, A. et al. Interprofessional education: tips for design and implementation. BMC Med Educ 20, 455 (2020). (Link)
Theoretical / Background Knowledge
These resources and activities summarize all topics from the student learning units to introduce educators to these concepts. These resources are part of the train-the-trainer courses and marked as "optional" . Thus, they can be used optionally by course facilitators if participants are not yet familiar with basic concepts.
Theme(s): All basic concepts of clinical reasoning Level: Educators Format: Additional resources and material provided for each train-the-trainer learning unit that can be integrated if needed, e.g. if participants are quite new to the topic. These resources cover the basic concepts of a topic without going into the teaching aspects, so they can be used as preparatory steps.
Metacognition, reflection and models for reflection
Similar to the novice learning unit learners are asked to complete a reflective diary for five days. However, in this learning unit they should focus on critical or difficult situations in the clinical context.
The learning unit includes the generation of a decision tree based on a breast cancer data set from radiology department using the RapidMiner software package and an elaboration of the concepts of sensitivity and specificity. Furthermore, we will apply Bayesian reasoning and give an opportunity to discuss the base rate fallacy problem and the use of electronic calculators to judge the risk. The learning unit is finished with a discussion of the barriers/facilitators of using computers/AI in hospitals to support clinical reasoning.
Theme(s): Gathering, interpreting, and synthesizing information, Decision making Level: Advanced Format: Synchronous meeting (ca. 90 min) followed by an asynchronous phase (ca. 90 min) Recommended ECTS: 0.1 Links: Student course - Facilitator resources
Uncertainty
In this learning unit, the approach of practice inquiry will be introduced and applied.
Theme(s): Biases & errors Level: Advanced Format: Asynchronous online preparation (ca. 60 min) followed by a synchronous meeting (ca. 60 min) Recommended ECTS: 0.07 Links: Student course - Facilitator resources
Analyzing and avoiding errors
This learning unit will provide general and specific aspects of a morbidity and mortality conference and apply the knowlege by working through a case report.
Theme(s): Biases & errors Level: Advanced Format: Asynchronous online preparation (ca. 60 min) followed by a synchronous meeting (ca. 90 min) Recommended ECTS: 0.08 Links: Student course - Facilitator resources
Biases and cognitive errors
This learning unit introduces additional errors and biases and your will have the opportunity to work on virtual patients to identify error-prone situations.
In this learning unit, learners will be familiarized or re-familiarized with the basic concept of shared decision-making (SDM) in a way that serves as a steping stone for how to implement key concepts and models into practice. A job aid on shared decision-making will be a takeaway from this learning unit.
Collaboration of health professions in clinical reasoning
In this learning unit you will be able to apply interprofessional aspects of clinical reasoning and understand similarities and differences between the clinical reasoning of health professions. This facilitates a better communicate across professions in the clinical reasoning process to meet the needs of the patient.
Theme(s): (Interprofessional) Collaboration Level: Intermediate Format: Starting with two synchronous meetings (each 60 min or combined) followed by an asynchronous follow-up (ca. 60 min) Recommended ECTS: 0.1 Links: Student course - Facilitator resources
Decision Support Systems
The aim of this learning unit is to facilitate a discussion about which aspects of clinical reasoning can be supported by artificial intelligence and what the limitations of machines in clinical reasoning are.
Theme(s): Gathering, interpreting, and synthesizing information, Decision making Level: Intermediate Format: Synchronous meeting (ca. 90 min) with a follow-up asynchronous phase (ca. 90 min) Recommended ECTS: 0.1 Links: Student course - Facilitator resources
Evaluation of Clinical Reasoning
This learning unit provides an overview about surveys and questions suitable to evaluate clinical reasoning teaching. It also introduces the relevance of learning analytics.
Theme(s): Teaching clinical reasoning Level: Educators Format: Self-guided on-demand course with different material on clinical reasoning evaluation (ca. 60 min) Recommended ECTS: 0.03 Links: Course
Discussing and teaching about cognitive errors and biases
In this learning unit participating educators and clinicians will have the opportunity to share ideas on how a culture for discussing errors should look like. They will also learn more about most common errors and biases in clinical resoning and (teaching) strategies on how to avoid these. This learning unit supports educators in teaching the student courses on the novice level: Biases and cognitive errors, Uncertainty, and Analyzing & avoiding errors
Theme(s): Teaching clinical reasoning, Errors & biases, Theories of clinical reasoning, Ethical aspects Level: Educators Format: Asynchronous preparation (ca. 60 min) followed by a synchronous meeting (ca. 90 min). Optional additional activities are provided for beginners (ca. 80 min). Recommended ECTS: 0.08 (including optional phase: 0.13) Links: Participant course - Facilitator resources
Information gathering, Generating differential diagonses, Decision making, and Treatment planning
This learning unit is designed to support educators in implementing the student courses on Collect and prioritize key clinical findings/problems, Generating differential diagnoses and deciding about final diagnosis, Developing a treatment plan, and Biomedical Knowledge and Clinical Reasoning
Theme(s): Teaching clinical reasoning, Gathering, interpreting & synthesizing information, Generating differential diagnoses, Developing a treatment / management plan, Decision making, Ethical aspects Level: Educators Format: Asynchronous preparation (ca. 60 min) followed by a synchronous meeting (ca. 60 min). Optional additional activities for beginners are available (ca. 60 min). Recommended ECTS: 0.07 (including optional phase: 0.1) Links: Participant course - Facilitator resources
Person-centred approach and the role of patients
This learning unit prepares educators to comprehensively and confidently teach the the learning unit on Person-centred approach to clinical reasoning. This unit will take educators through the learning content provided in the learning unit, as well as supports them in familiarizing themselves with the resources and exercises. Educators will have the opportunity to create their own teaching notes as part of this learning unit.
Theme(s): Teaching clinical reasoning, Patient perspective Level: Educators Format: Asynchronous preparation (ca. 60 min), followed by a synchronous meeting (ca. 90 min). Optional additional activites are available for beginners (ca. 100 min). Recommended ECTS: 0.08 (including optional phases: 0.14) Links: Participant course - Facilitator resources
Differences and similarities in clinical reasoning among health professions
This learning unit introduces teaching methods for clinical reasoning in different healthcare professions and prepares educators to teach the learning units on Health profession roles in clinical reasoning
This learning unit familiarizes healthcare profession educators on teaching aspects related to the clinical reasoning process and terminology of the different health professions. This includes how to explain the importance of clinical reasoning in the different health professions to students and how to support students in reflecting on clinical reasoning theories. The learning unit prepares you for teaching the novice courses on What is clinical reasoning, Dual Process Theory, Outcome Present State model, and Illness scripts.
Theme(s): Teaching clinical reasoning, Theories of clinical reasoning Level: Educators Format: Two synchronous meetings (ca. 60 and 45 min) with asynchronous phase (ca. 45 min) in between. Optional additional phase with ca. 45 min. Recommended ECTS: 0.08 (including optional phase: 0.11) Links: Course, Facilitator resources
Clinical Reasoning teaching and assessment
This learning unit provides and overview about teaching and assessment methods for clinical reasoning. It also highlights some general apsects, such as the importance of constructive alignment or how to organize group discussions.
Theme(s): Teaching clinical reasoning Level: Educators Format: Self-guided on-demand course with different material on clinical reasoning teaching and assessment. Recommended ECTS: 0.03 Links: Course
This learning unit provides an overview about the DID-ACT student curriculum including all course outlines and resources neede to implement these learning units. It also introduces a tutorial on how to read the course outlines and use the provided resources.
Theme(s): Teaching clinical reasoning Level: Educators Format: Self-guided on-demand course with different material on our DID-ACT curriculum including all course outlines for student learning units and material needed. Links: Course
Analyzing and avoiding errors
Along a case report this learning unit introduces the root cause analysis (RCA) to analyze errors and start to find ways for preventing / avoiding errors.
Theme(s): Errors & Biases Level: Novice Format: Asynchronous preparation (ca. 90 min) followed by a synchronous meeting (ca. 70 min) Recommended ECTS: 0.09 Links: Student course - Facilitator resources
Metacognition, reflection and models for reflection
In this learning unit reflection models will be introduced and self-reflection will be applied on form of a reflective diary.
Theme(s): Errors & biases Level: Novice Format: Synchronous meeting (ca. 60 min), followed by an asynchronous online phase (ca. 80 min) and a concluding synchronous meeting (ca. 80 min) Recommended ECTS: 0.12 Links: Student course - Facilitator resources
Uncertainty
The aim of this learning unit is to introduce situations of uncertainty and strategies that can be applied in such situations to avoid errors.
Theme(s): Errors & biases Level: Intermediate Format: Asynchronous preparation (ca. 60 min) followed by a synchronous session (ca. 90 min) Recommended ECTS: 0.08 Links: Student course - Facilitator resources
Biases and cognitive errors - an Introduction
This learning unit provides a basic introduction into the topic of biases and cognitive errors. It introduces a selection of common biases, such as premature closure or confirmation bias with providing the opportunity to elaborate on these biases with case vignettes.
This learning unit provides an introduction into the topics "EBM in the context of clinical reasoning" and "developing a treatment/management plan" for students with no or some prior clinical experience.
Theme(s): Developing a treatment / management plan, Ethical aspects, Patient perspective Level: Novice Format: Asynchronous preparation (ca. 45 min) followed by a synchronous meeting (ca. 80 min) Recommended ECTS: 0.08 Links: Student course - Facilitator resources
Generating differential diagnoses and deciding about final diagnosis
This learning unit introduces different methods of creating and organizing differential diagnoses. There is also opportunity to practice the finding of differential diagnoses as well as discriminating and confining features on a prototypical case.
Theme(s): Generating differential diagnoses, Decision Making Level: Novice Format: Two synchronous meetings (ca. 90 min each) with an asynchronous phase in between (ca. 60 min) Recommended ECTS: 0.13 Links: Student course - Facilitator resources
Collect and prioritize key clinical findings/problems
This learning unit highlights how to collect and prioritize key clinical findings using case examples.
Theme(s): Gathering, interpreting & synthesizing information Level: Novice Format: Asynchronous preparatory phase (ca. 45 min) followed by a synchronous meeting (ca. 60 min) Recommended ECTS: 0.06 Links: Student course - Facilitator resources
Biomedical Knowledge and Clinical Reasoning - Knowledge Encapsulation
This learning unit explains the interconnection of biomedical knowledge and differential diagnoses formulation and explores different techniques to visualize encapsulated knowledge.
Theme(s): Theories of Clinical Reasoning Level: Novice Format: Two synchronous sessions (ca. 60 min each) with an asynchronous learning phase in between (ca. 45 min) Recommended ECTS: 0.09 Links: Student course - Facilitator resources
Person-centered approach to clinical reasoning
The goal of this learning unit is to define what a 'person perspective' is in the context of healthcare provision and highlight why it is important when providing a quality healthcare experience. Learners will also visit the definitions of biomedical information as well as recite the terminology "diagnostic and analysis" in a way that helps patients and their families understand this stage in healthcare provision. Lastly, learners will combine the above into practical ability using questions that promote support for families and patients using terminology that facilitates mutual understanding.
Theme(s): Patient perspective Level: Novice Format: A synchronous meetings (ca. 90 min), with a preparatory and a follow-up asynchronous phase (ca. 90 and 45 min) Recommended ECTS: 0.13 Links: Student course - Facilitator resources
Collaborate with others in clinical reasoning
This learning unit provides basic knowledge within different healthcare professions or across medical specialisations e.g. surgery, internal medicine and their collaboration with others in clinical reasoning.
This learning unit provides an introduction to the various health professions involved in health care on the subject of clinical reasoning. The unit has been developed for beginner and novice learners, and is appropriate for those who have and have not yet had extensive clinical experience due to the team aspect of the assessments. The learning unit will highlight varied professions ranging between physiotherapy, medicine, nursing, and occupational therapy and learners will be able to compare and contrast the definitions of clinical reasoning within said professions, as well as relate how this team-understanding fits into the broader picture of healthcare, with a goal to establish a common understanding and definition of 'clinical reasoning'.
Theme(s): (Interprofessional) Collaboration Level: Novice Format: Asynchronous preparatory phase (ca 45 min) followed by a synchronous meeting (ca. 90min) Recommended ECTS: 0.08 Links: Student course - Facilitator resources
Using the Outcome Present State Test Model
This learning unit provides an introduction into the the Outcome-Presenter-State model for clinical reasoning, which is applied especially in nursing. The learning unit is designed for novices of all health professions who are at the beginning of their education.
This learning unit provides an introduction into scripts in general and more specifically into llness scripts for novices who are at the beginning of their education and do not have any prior knowledge or experience with illness scripts.
Theme(s): Theories of Clinical Reasoning Level: Novice Format: Two synchronous sessions (ca. 160 min) with an asynchronous learning phase (ca. 60 min) in between Recommended ECTS: 0.12 Links: Student course - Facilitator resources
Dual Process Theory
This learning unit provides an introduction into the dual processing theory amd highlights the differences between system 1 and system 2 reasoning.
Theme(s): Theories of Clinical Reasoning Level: Novice Format: Asynchronous preparation phase (ca. 90 min) followed by a synchronous meeting (ca. 90 min) Recommended ECTS: 0.1 Links: Student course - Facilitator resources
What is clinical reasoning and how can theories be put into practice
This learning unit covers how clinical reasoning theories can be used/applied during beside teaching, internships or other patient-centered situations and why it is important to know these theories. It deepens the differences and similarities of clinical reasoning in the health professions, terminology used and importance of clinical reasoning.
Theme(s): Theories of Clinical Reasoning Level: Intermediate Format: Asynchronous preparation (ca. 45 min) for a follow-up synchronous meeting (ca. 60 min) Recommended ECTS: 0.07 Links: Student course - Facilitator resources
What is Clinical Reasoning - An Introduction
This learning unit provides an introduction into the topic for novices who are at the beginning of their education and do not have any prior knowledge or experiences with clinical reasoning.
Theme(s): Theories of Clinical Reasoning Level: Novice Format: Synchronous meeting (60 min) followed by asynchronous follow-up (60 min) RecommendedECTS: 0.07 Links: Student course - Facilitator resources